
Clinical Quality & Safety
SJMC Clinical Quality & Safety Results
At SJMC, we are committed to providing high-quality care and maintaining the safety of our patients. Our clinical quality and safety results highlight our dedication to excellence in healthcare services. We continuously monitor and improve our performance across various departments, ensuring that patients receive care that meets or exceeds national and global standards.
Our Data & Results
Hospital-Wide Quality & Safety Results
Hand Hygiene Indicators
What SJMC does to reduce your risk?
In SJMC, we aim to minimise the risk of infection to patients, staff and visitors that come to our hospital.
What you can do to reduce your risk?
There are several ways you can assist in preventing an infection:
- Always wash your hands after using the toilet, bedpan or a commode
- Wash or clean your hands before eating
- Don’t be afraid to ask your doctor or staff caring for you, if they have washed their hands
- Avoid touching your wound or devices (for example, fluid tubes into your arm or drain tubes)
- Let the care staff know if your wound or areas around any of the lines or tubes become red or swollen or painful
- Discourage visitors who may be feeling unwell
- Stop smoking before any surgery, as smoking increases the risk of infection
One of the most effective ways to prevent infection spreading amongst patients is for all health professionals to wash their hands. Hand hygiene is conducted in accordance with the ‘five moments’ that are: before touching a patient; before a procedure; after a procedure; after touching a patient; and after touching a patient’s environment.
SJMC participates in the WHO hand hygiene strategy, and hand hygiene audits are conducted regularly.
Hand hygiene compliance is reported as the percentage of correct moments from all observed moments.
Hand Hygiene Compliance (A higher rate is better)
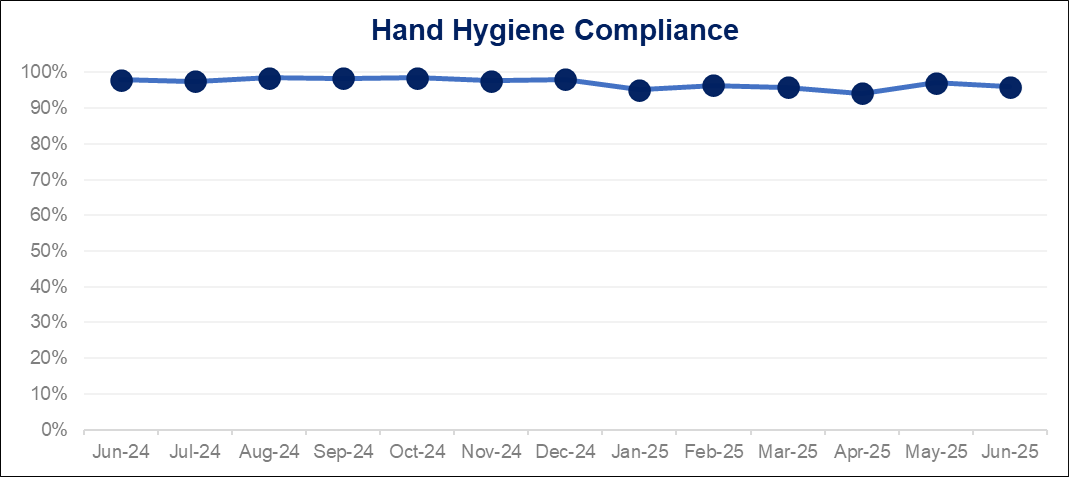
| Quality Indicators Description | SJMC Results Jan to Jun 2024 | SJMC Results jul to Dec 2023 | SJMC Results Jan to Jun 2025 | Healthcare Industry Published Rates |
|---|---|---|---|---|
Overall Hand Hygiene Compliance | 97% | 98% | 96% | Malaysia Patient Safety Goals Target:>75% |
Inpatient Falls | 0.05% | 0.040% | 0.043% | 0.3% 2 |
| SJMC use a number of strategies to prevent falls and these include ensuring that call bells and personal items are within the patient’s reach and patients are assisted to the toilet at regular intervals. In addition, we have implemented patient alarms to minimise the risk of adult patients falling while admitted. | ||||
- SJMC participates in the Australian Council on Healthcare Standards (ACHS) Clinical Indicator Program and use their definitions for these indicators. This program provides a national clinical benchmarking service and is comprised of comparative information on the processes and outcomes of health care.
- Australian Council on Healthcare Standards (ACHS). ACHS Clinical Indicator Report: 2016–2023 25th Edition Sydney, Australia; ACHS; 2024.
Concerned about Quality and Safety? Click here to make a report.